
Diabetes & Your Eyes
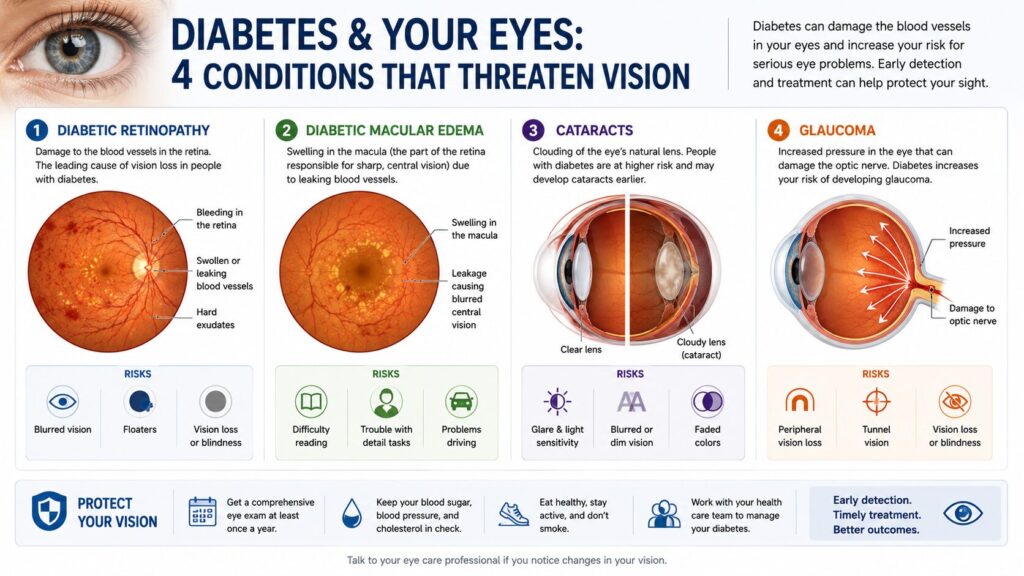
Diabetes and Your Eyes describes the relationship between chronically elevated blood sugar and four distinct eye conditions: diabetic retinopathy, diabetic macular edema, glaucoma, and cataracts that develop silently and can cause permanent vision loss if left undetected. Unlike most diabetes complications, eye damage often produces no pain and minimal symptoms until it’s advanced.
That’s exactly what makes it dangerous.
What High Blood Sugar Actually Does to Your Eyes
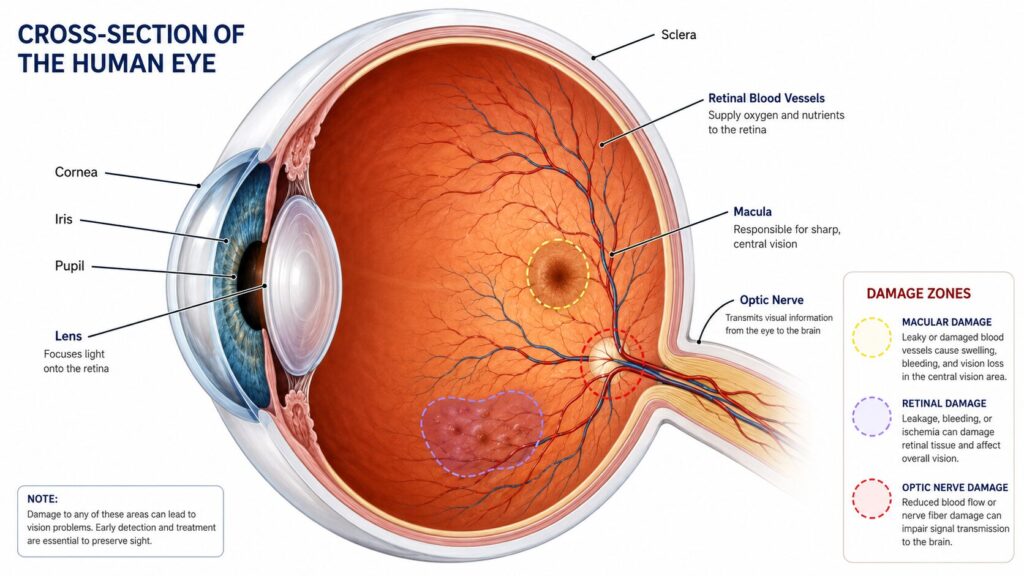
Your retina is lined with a dense network of tiny blood vessels some of the smallest in the entire body. When blood glucose stays elevated for months or years, those vessels weaken, swell, leak fluid, and eventually close off entirely. The retina then sends distress signals that trigger the growth of new, fragile replacement vessels. These new vessels bleed easily. That’s the core mechanism behind most diabetic eye disease.
Here’s the thing: the damage starts before you notice it. There’s no pain. There’s no obvious blurriness at first. By the time vision changes are obvious enough to bring someone to a clinic, the disease has often been active for years.
According to a 2024 study published in JAMA Ophthalmology and reported by the CDC’s Vision and Eye Health Surveillance System, an estimated 9.6 million Americans 26.4% of all people with diabetes were already living with diabetic retinopathy in 2021. Of those, 1.84 million had vision-threatening disease. The number of people 40 and older with diabetes-related eye damage more than doubled since it was last measured in 2004.
Most people assume blurry vision from diabetes is temporary caused by blood sugar swings. Sometimes it is. But persistent or worsening blur is a different story entirely.
The 4 Diabetic Eye Conditions, Explained Separately
This is what most general diabetes articles skip. They mention “eye problems” as a single bullet point. But there are four distinct conditions, each with its own mechanism, staging, and treatment window and you can have more than one at the same time.
Diabetic Retinopathy
Diabetic retinopathy is damage to the blood vessels of the retina caused by prolonged high blood sugar. It’s the leading cause of new blindness in adults aged 20–74 in developed countries, according to the American Diabetes Association’s 2025 Standards of Care.
It progresses in two stages:
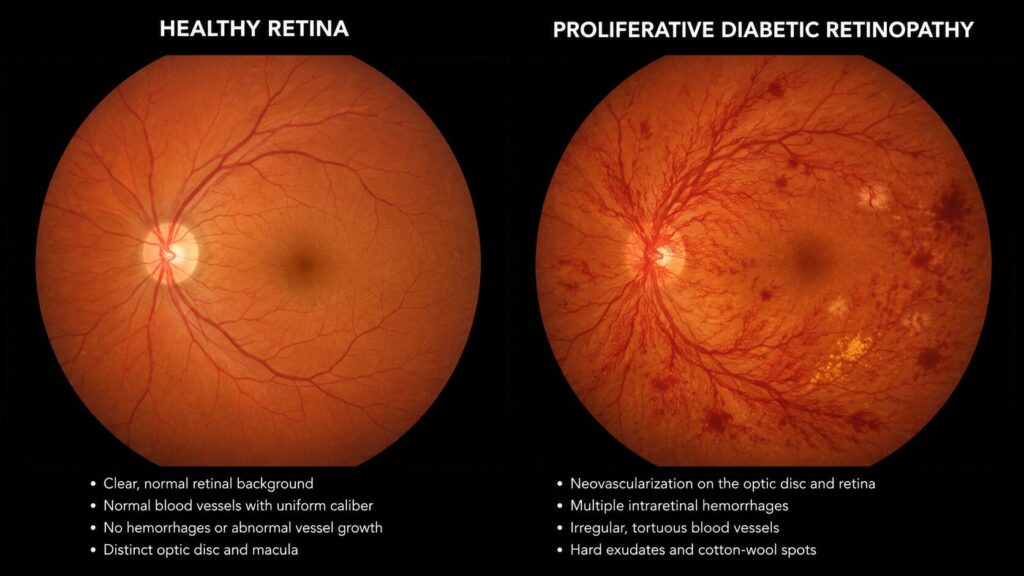
- Non-proliferative diabetic retinopathy (NPDR): Blood vessels leak fluid and small bulges (microaneurysms) form. Vision may still be normal. This is the stage where early intervention is most effective.
- Proliferative diabetic retinopathy (PDR): New abnormal blood vessels grow across the retina and into the vitreous. These bleed easily, causing sudden dark spots or floaters. Retinal detachment becomes a real risk.
Risk goes up sharply with diabetes duration. After 20 years with Type 1 diabetes, nearly all patients show some retinopathy. With Type 2, the timeline is less predictable which is why screening from diagnosis is non-negotiable.
Diabetic Macular Edema
Diabetic macular edema (DME) is fluid buildup in the macula the central part of the retina responsible for reading, driving, and recognizing faces. It can occur at any stage of retinopathy, including early stages.
DME is the most common cause of vision loss in people with diabetes.
The primary treatments are anti-VEGF injections medications that block the vascular growth factor driving leakage. The two most widely used are Eylea (aflibercept) and Lucentis (ranibizumab), both FDA-approved for DME. A 2024 study in Ophthalmology Retina tracking over 124,000 eyes found that patients receiving anti-VEGF injections gained an average of 3.2 letters of visual acuity at one year. Not dramatic but the goal is to stop the loss, not just improve it.
A newer option worth knowing about: Susvimo, a refillable eye implant that delivers ranibizumab continuously, reducing treatment visits from monthly to twice a year. A 2024 clinical study showed comparable vision outcomes to monthly injections.
Quick note: laser therapy (focal photocoagulation) is still used when anti-VEGF doesn’t fully resolve the edema or when injections aren’t an option for example, during pregnancy.
Glaucoma
People with diabetes are roughly twice as likely to develop glaucoma compared to people without it. The most diabetes-specific form is neovascular glaucoma, where the same abnormal new blood vessels that grow on the retina also block the eye’s drainage system, causing dangerous pressure buildup.
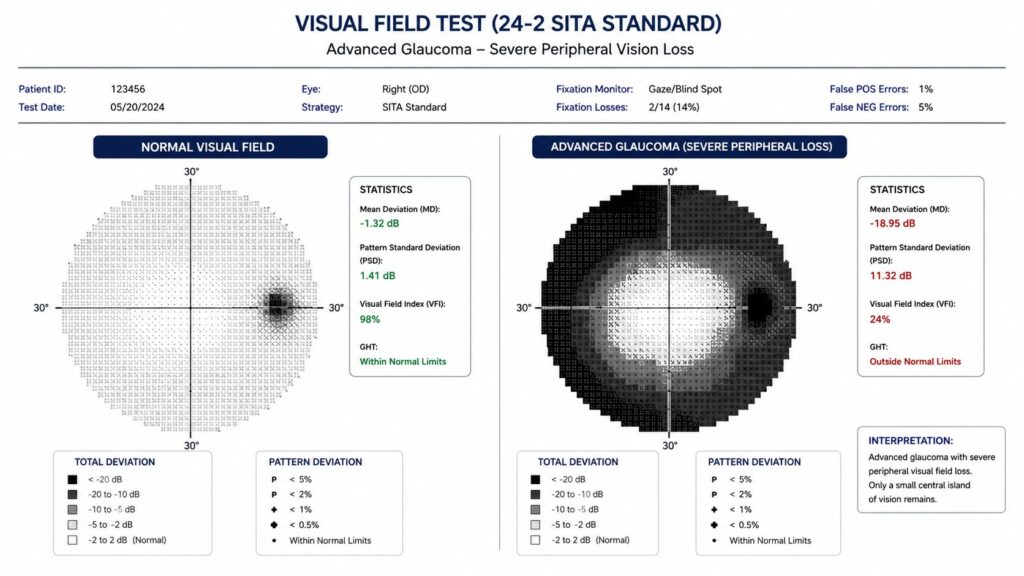
Treatment ranges from eye drops that lower intraocular pressure to laser procedures to surgical drainage implants. The challenge: glaucoma damage to the optic nerve is permanent. Early detection is everything here.
Cataracts
Cataracts clouding of the eye’s natural lens happen in everyone with age. But in people with diabetes, they happen earlier and progress faster. Elevated glucose causes chemical changes in the lens proteins, accelerating the clouding process.
Cataract surgery (lens replacement with an artificial intraocular lens) is highly effective. The catch: in diabetic patients, retinopathy can actually worsen after cataract removal, and the surgical inflammation can trigger or accelerate macular edema. Your surgeon needs to know your full retinal history before operating.
Quick Comparison: The 4 Diabetic Eye Conditions
| Condition | Best Detected By | Primary Treatment | Key Risk If Missed |
|---|---|---|---|
| Diabetic Retinopathy | Dilated retinal exam / Optos imaging | Anti-VEGF injections, laser | Retinal detachment, blindness |
| Diabetic Macular Edema | OCT scan (optical coherence tomography) | Eylea, Lucentis injections | Permanent central vision loss |
| Neovascular Glaucoma | Tonometry + gonioscopy | Eye drops, laser, surgery | Irreversible optic nerve damage |
| Cataracts | Slit-lamp exam | Surgical lens replacement | Progressive vision loss |
Your Diabetic Eye Exam Schedule (Based on Diabetes Type and Duration)
This is the section that competitor articles consistently leave out. Here’s a concrete schedule based on the American Diabetes Association’s 2025 Standards of Care:
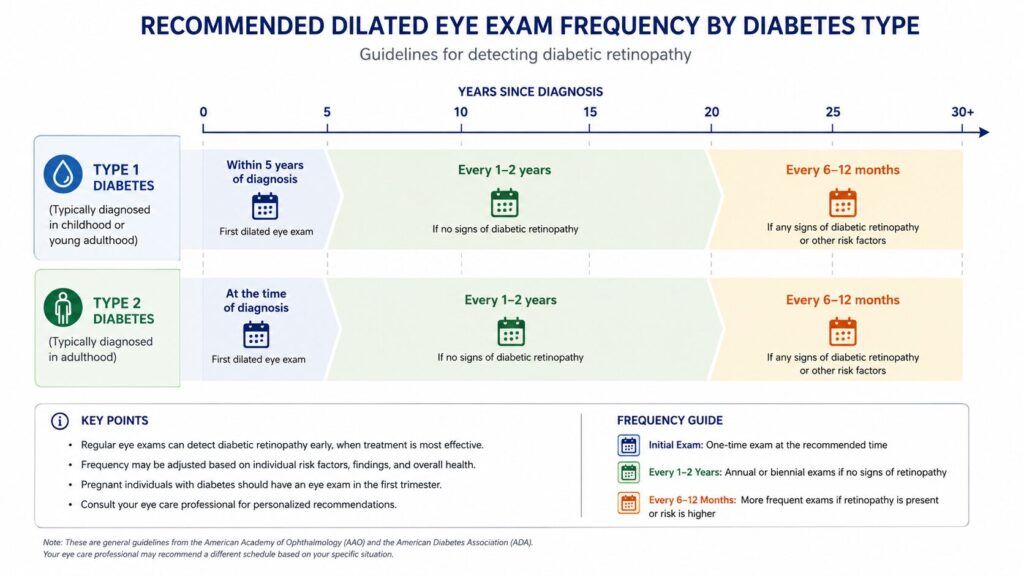
To protect your vision as a person with diabetes, follow this exam schedule:
- Type 1 diabetes: Get your first dilated eye exam within 5 years of diagnosis.
- Type 2 diabetes: Get your first dilated eye exam at the time of diagnosis not later.
- No retinopathy found: Annual exams every 1–2 years, depending on your doctor’s assessment.
- Retinopathy present: Exams every 6–12 months, sometimes more frequently during active disease.
- Pregnancy with diabetes: Get examined in the first trimester retinopathy can worsen rapidly during pregnancy.
Look if you’ve had Type 2 diabetes for more than 5 years and haven’t had a dilated exam yet, that’s the one thing you should do this week. Not next month.
What to ask for: A standard eye exam isn’t enough. You need a dilated fundus exam where drops widen your pupil so the doctor can see your full retina. Many practices now also offer Optos ultra-widefield retinal imaging, a technology that captures up to 82% of the retina in a single photograph without dilation, or with minimal dilation. It’s increasingly used as a supplement or alternative, though the American Diabetes Association still recommends dilation as the gold standard for comprehensive screening.
Can You Actually Prevent Diabetic Eye Disease?
Or maybe I should say it this way can you prevent it, or can you only slow it down? The answer depends on where you are in the disease process.
Before damage starts: Yes, genuinely preventable. Multiple large studies including the landmark DCCT trial for Type 1 and UKPDS for Type 2 showed that tight glycemic control significantly reduces the risk of developing retinopathy. Controlling blood pressure matters nearly as much as blood sugar. The 2025 ADA Standards of Care also note that GLP-1 receptor agonists (medications like semaglutide, now widely prescribed) may reduce intraocular pressure and lower glaucoma risk.
After damage starts: Progression can often be slowed or halted. Some stages of retinopathy can stabilize completely with improved glucose and blood pressure control. That’s not nothing that’s the difference between keeping functional vision and losing it.
I’ve seen conflicting data on exactly how much A1C reduction corresponds to retinopathy risk reduction across different populations some trials show dramatic benefit from even modest improvements, while others show more modest effects in long-duration disease. My read is that the benefit is real and clinically significant in most patients, particularly in the first decade of diabetes.
Some experts argue that aggressive blood sugar control is always the priority over everything else. That’s valid for most patients. But if you’re dealing with very long-duration diabetes or you’ve already experienced a rapid drop in A1C after years of poor control a paradoxical short-term worsening of retinopathy called “early worsening” has been documented. Your ophthalmologist and endocrinologist need to coordinate in that scenario.
What Symptoms Actually Mean — and What to Watch For
Most people with early diabetic eye disease have no symptoms at all.
That bears repeating: no symptoms.
When symptoms do appear, they can include:
- Blurry or fluctuating vision (often the first complaint and often dismissed as needing a new glasses prescription)
- Dark spots, floaters, or “cobwebs” drifting across vision
- A dark or empty area in the center of your visual field (macular edema)
- Sudden, painless vision loss in one eye (vitreous hemorrhage a medical emergency)
- Difficulty with color perception, particularly distinguishing blues and purples
Fluctuating blur that tracks with blood sugar levels worse when sugar is high, better when controlled is usually osmotic, caused by the lens swelling slightly. It typically resolves with better glucose management. Persistent blur that doesn’t track with sugar levels is a different signal and warrants prompt evaluation.
What Most Guides Skip: The A1C–Eye Damage Connection Is Not Linear
What most guides skip is that the relationship between your A1C and your eye risk isn’t a simple straight line.
Duration of diabetes is often a stronger predictor of retinopathy than current A1C alone. Someone who has had Type 2 diabetes for 15 years with an A1C of 7.5% may have more retinal damage than someone newly diagnosed with an A1C of 10% because cumulative exposure matters. This is why screening from the moment of Type 2 diagnosis is so important, regardless of how “controlled” you feel your diabetes is.
The other underreported factor: blood pressure. Hypertension accelerates retinal vascular damage independently of blood sugar. The 2025 ADA Standards note that lowering blood pressure slows retinopathy progression though targeting very strict systolic goals below 120 mmHg doesn’t add additional benefit beyond standard control.
Voice Search Q&A
Q: What’s the best way to protect your eyes if you have diabetes?
A: Get a dilated eye exam at diagnosis (Type 2) or within five years (Type 1), then annually. Control blood sugar, blood pressure, and cholesterol all three drive retinal damage independently.
Q: How do I know if diabetes is affecting my eyes?
A: Often you won’t early diabetic eye disease has no symptoms. Persistent blurry vision, dark floaters, or a blank spot in your central vision are warning signs that need immediate evaluation.
Q: Should I see an eye doctor even if my vision seems fine?
A: Yes. Diabetic retinopathy causes no pain and little noticeable vision change until it’s advanced. Annual dilated exams catch damage before it becomes vision-threatening.
Q: Why does diabetes cause blurry vision?
A: Short-term blur is caused by blood sugar fluctuations making the eye’s lens swell. Long-term, diabetes damages retinal blood vessels, causing leakage, swelling in the macula, and eventually new abnormal vessel growth.
Q: When should I go to the ER for diabetes-related eye symptoms?
A: Sudden painless vision loss, a large shower of floaters, or a dark curtain across any part of your vision are emergencies. These can signal vitreous hemorrhage or retinal detachment call your ophthalmologist or go to the ER immediately.
This article covers established eye complications of Type 1 and Type 2 diabetes in adults. It does not address diabetic cranial nerve palsies, contact lens complications in diabetics, or insurance coverage for diabetic eye screenings.
